Performance overview 2025-26
Performance overview 2025-26
Chief Executive’s introduction: a year of delivery, momentum and system leadership
2025-26 was a defining year for health and social care research in the UK, and for the Health Research Authority’s role within it.
It was a year in which strong delivery was matched by growing momentum across the system, and where sustained system leadership translated into clear advantages for UK citizens and UK research.
The year opened with a clear national ambition. The Prime Minister challenged the system to reduce the time to set-up a clinical trial in the UK to 150 days, placing renewed emphasis on pace, predictability and confidence for researchers and sponsors, which in turn translates into more research happening in the UK to benefit UK patients and the UK economy. We’ve been working with partners as part of the DHSC-led UK Clinical Research Delivery (UKCRD) programme to deliver the changes that are needed to achieve this 150 day target. On 15 April 2026 the UK government announced that we had achieved that target.
At the same time, we continued to deliver consistently against our own statutory responsibilities. For the second consecutive year, we met our monthly target of issuing a final ethics opinion on 100% of all clinical trials of investigational medicinal products (CTIMPs) in England within 60 days of submission. This sustained performance matters: it provides a stable, reliable foundation on which wider system improvements depend.
Building on this momentum, in July 2025, we launched the new HRA Strategy 2025-28, Boosting research that improves health and grows the economy, setting out how the HRA’s work supports the national missions on health and growth. While our mission remains unchanged - to make it easier to do research that people can trust – the strategy makes explicit our role as a system enabler and leader, working with others to improve how research is planned, approved and delivered across the UK.
Turning that strategy into delivery was a major focus during the year with momentum across clinical research further strengthened by the government’s commitment to “turbocharge” clinical trials, underpinned by significant investment in digital infrastructure.
The Integrated Research Application System (IRAS) is the single system for applying for permissions and approvals for health, social and community care research in the UK. In December 2025, we celebrated a significant milestone with the first live use of the new ‘Plan and Manage Health and Care Research’ service, marking the beginning of the transformation of IRAS. For the first time, a small, invited cohort of users were able to test the service to manage changes to active studies. This represents the start of a wider shift towards a simpler, more joined-up digital experience for researchers, with further progress planned through 2026 and 2027 as we design services for research that is not a clinical trial of an investigational medicinal product (CTIMP) and then CTIMPs. Throughout this programme, involving the users of the system – researchers, committee members and staff – in the development of new services has been fundamental to developing a world leading system that we are all proud of.
As the year drew to a close, we prepared for the most significant reform to UK clinical trials regulation in a generation to come into force. In April 2026, the updated clinical trials regulations became law, making the culmination of a year-long transition, and more than 3 years of sustained, collaborative work between the HRA and the Medicines and Healthcare products Regulatory Agency (MHRA), in partnership with other organisations across the UK.
The new regulations fundamentally reset how clinical trials of medicines are regulated in the UK. They enable faster and more predictable approvals, apply proportionate regulation based on risk and strengthen both transparency and inclusion. Together, these changes are central to delivering the UK government’s ambition to reduce clinical trial set-up to 150 days, while reinforcing the UK’s position as a trusted and globally competitive environment for clinical research.
Throughout 2025–26, our focus was on supporting researchers and sponsors to prepare for this change. We developed detailed guidance shaped directly by feedback from the research community, recognising that the real value of regulatory reform lies in how confidently and consistently it can be applied. The successful introduction of the new regulations illustrates the UK system at its best: progress driven by shared purpose, partnership and clear system leadership.
Alongside pace and efficiency, trust remained at the heart of our work.
High‑quality research must be transparent, involve the public meaningfully, and include participants from across society. In October 2025, we brought together more than 300 people from across the research community at our research transparency event, focused on improving how results are shared with participants. Over the year, we also strengthened how we collect and analyse final report data, enabling us to provide a clearer picture of transparency compliance and laying the groundwork for a new research transparency strategy to be published in 2026-27. In April 2026, we published our latest data showing that more studies than ever are registered on a public registry (94%), but that only half of studies completed in 2023 have shared their results with participants. This shows great progress on registration, but we need to harness that momentum to improve the research transparency metrics for publication of results and for feeding back to participants.
This year also saw the publication of the final report of the Infected Blood Inquiry. Its findings were sobering and serve as a powerful reminder of what can go wrong when independent oversight and transparency are absent. The infected blood scandal was a tragedy that must never be repeated. While the research governance environment has changed profoundly since then, not least with the creation of the HRA, we must not be complacent. These historic failings continue to risk undermining trust in clinical research today, making it essential that the HRA and the wider research community continue to earn and maintain public confidence. The Inquiry made 2 recommendations specifically for the HRA. The first asks us to work with the National Institute for Health and Care Research (NIHR) and with research participants to update the 2014 framework on sharing health‑related findings with people involved in research, reflecting significant changes in access to health information and public expectations. The second recommends developing a clear, user‑friendly explanation of participants’ rights and responsibilities, including how concerns can be raised and addressed. We accepted both recommendations unreservedly and will take this work forward in the year ahead.
None of this work would be possible without the commitment of our staff and volunteers.
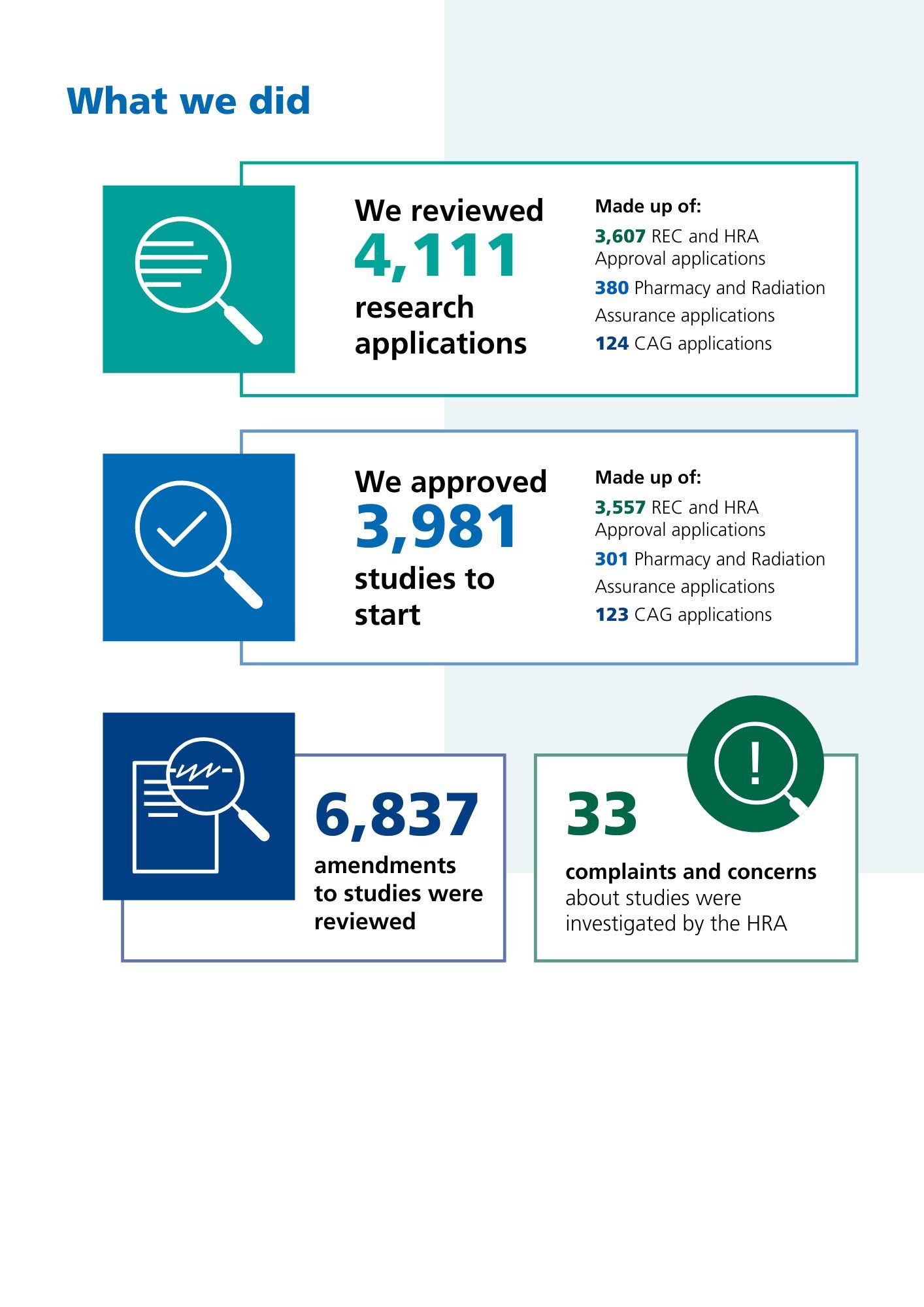
Our Research Ethics Committees (RECs) provided opinions on 3,607 new research projects this year, which equates to more than 9 a day. We now have nearly 900 REC members, and ably supported by our staff, they have also ensured that more than 6,000 substantial amendments were reviewed this year too – 92% of which were within 35 days, which is a phenomenal achievement. Our Confidentiality Advisory Group (CAG), who provide expert advice on the use of confidential patient information for purposes beyond patient care, reviewed 124 applications, and welcomed a new Chair and Vice Chair this year.
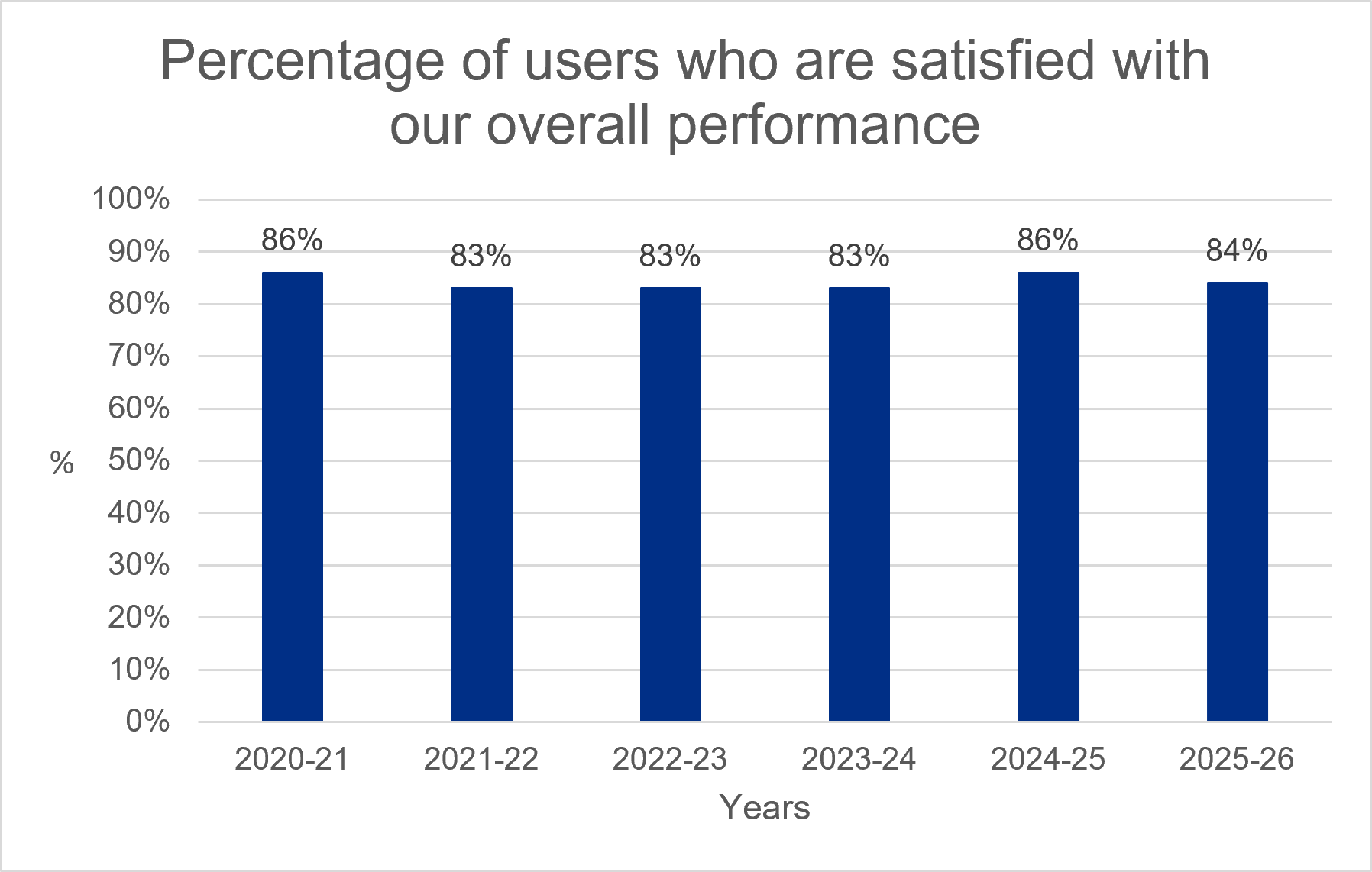
Our staff continually receive high satisfaction scores based on surveys we conduct with our research community, as detailed below, and of this I am immensely proud.
I’ve been delighted to welcome some new faces to our Board this year, who have helped oversee this new direction. In July 2025, Neelam Patel was appointed as our permanent Chair, and in February 2025 we welcomed 3 new Non-Executive Directors - Professor Alastair Denniston, Professor Marian Knight MBE and Dr Mark Buswell. We also welcomed Dr Jonathan Fennelly-Barnwell as Interim Director of Approvals, after we said goodbye to Dr Janet Messer, his predecessor, earlier this year. In 2026-27, we will be joined by an additional non-executive director later this year, and will be advertising for a substantive replacement for our Director of Approvals.
Looking ahead, the pace of change, delivery, momentum and system leadership, will continue. We will be convening an important conversation on how we embed the fantastic effort leading to delivery of the PM’s 150 day target for long-term sustainability and providing a world class, UK-wide experience for investors, researchers and participants. We will be working on a new operating model for the HRA, and working in partnership with colleagues in all 4 nations of the UK, on a new proposal for how health and social care research is approved and delivered. We will support that through continued delivery of our digital transformation through further releases of Plan and Manage Health and Care Research. The growing use of artificial intelligence in research, alongside rising volumes and complexity of applications, will require continued clarity about how innovation can be enabled safely and ethically. The National Commission into the Regulation of AI in Healthcare, led by the MHRA and co‑chaired by our Non‑Executive Director Professor Alastair Denniston, will play an important role in shaping that next phase. We ourselves will be publishing our plan for AI in the next few months.
This year demonstrated what can be achieved through delivery, momentum and system leaders working together. I would like to thank everyone who has worked with us and look forward to building on that progress and partnership in the year ahead

Chief Executive, Health Research AuthorityDr Matt Westmore

Key issues and risks
As with all organisations, there are risks that we face while we make our strategy happen. We actively and effectively manage these to minimise any impact on users of our services, as well as other stakeholders and our people. Page 40 gives more detail about our risk management system.
Our strategic risk register was updated and refreshed this year to reflect our new strategy. This register was developed with involvement from our Executive Committee and Audit and Risk Committee before being approved at the March 2026 Board meeting. We score risks on a scale from 1 to 25, where higher scores mean the risk is more likely to happen and could have a greater impact. The residual risk score shows the level of risk that remains after we have taken steps to reduce it, such as putting controls or actions in place. It reflects the risk we are still managing, rather than the risk before any action was taken.
The Audit and Risk Committee and Board review the strategic risk register every 3 months. The HRA has 6 main strategic risks which are summarised as follows:
Supporting UK growth in life sciences
The HRA may not fully achieve its aim to support growth in life sciences with it facing several strategic and operational risks across its core mission areas. This could be due to inadequate digital infrastructure, resource constraints, policy misalignment, cybersecurity and data governance threats and stakeholder confidence.
The effect of this could lead to slower production of research evidence and in turn, the development and approval of new treatments and technologies, or adoption of new standards. It could lead also to a loss of investment, an erosion of trust, a negative perception of the UK’s research environment and therefore a failure to meet government priorities
How we make our strategy happen is a key control to manage this risk with the Board regularly sighted on progress. We have changed how we plan our activities to focus on strategy outcomes and work to review and realign our target operating model has commenced. We are focused on better aligning work to achieve our strategy outcomes and minimise the likelihood of this risk occurring.
The residual risk currently scores 12 on a scale from 1 to 25.
Helping reduce health inequalities
The HRA may not fully achieve its aim to help reduce health inequalities because it faces a range of risks. These include strategic, reputational, and operational risks. This could happen if research policy, funding decisions, or priorities are not inclusive, if research is not designed or carried out in ways that reflect everyone’s needs, or if our work is not well aligned with national health priorities. These risks could also arise if there is not enough collaboration, if people perceive bias or unfairness or if there is a lack of openness and transparency.
If this risk occurs, it could make existing health inequalities worse. Some people may have less access to research and opportunities to improve health outcomes could be missed. This could also damage our credibility, lead to perceptions of bias or exclusion, attract criticism from advocacy groups and reduce our influence.
Trust in research is a key part of our strategy. To manage this risk we have undertaken work to better understand who our different stakeholders are, what they know about us and would like from us. This will inform our work over the next two years of the strategy to ensure that the people that need us can find us, understand and trust us, and get the information that they need when they need it.
The residual risk currently scores 6 on a scale of 1 to 25.
Increasing the impact of money invested
The HRA may not fully achieve its aim of increasing the impact of money invested in health and social care research as it faces a range of strategic, reputational, operational, and systemic risks. These include insufficient acceleration of research processes, challenges in our digital transformation, transparency and reporting gaps and public confidence disparities.
If the research system is fragmented and there is no shared, joined-up approach to efficiency and productivity - including how work is prioritised and reported - this could reduce the value gained from public investment. It could also make it harder to deliver research that supports national health priorities. Over time, this could lead to a loss of public trust, less engagement from key stakeholders and could weaken the UK’s position as a competitive place to carry out research competitiveness.
We have introduced a strategy information sharing group to manage this risk to enable an aligned understanding of what is happening across the HRA to make our strategy happen. It enables rapid organisational awareness, connects activities, strengthens cross-team collaboration, provides space for clarification and reinforces transparency. We will also embed productivity and efficiency within our business planning and benefits processes and make sure we improve our understanding of the value the HRA and research contributes to better inform investment decisions.
The residual risk currently scores 12 on a scale of 1 to 25.
Digital
Robust and scalable digital systems are essential to helping the HRA do its work well and maintain progress over time. If the HRA does not have the right digital systems in place, particularly systems that support joined-up research applications processes, it may struggle to achieve its strategy. This could happen because of outdated systems, historic underinvestment in digital improvements, skills and capacity gaps, weak change management or risks linked to cybersecurity and data handling.
If this risk occurs, it could lead to slower research approvals, inefficient use of public resources, less transparency and poorer access to reliable data.
To manage this risk, we have made strong progress with our Research Systems programme which is modernising our digital services. In December 2025, we reached an important milestone with the first live use of the new Plan and Manage Health and Care Research service with users able to access a modern service to manage changes to active studies.
Over the year, we also reviewed and updated our existing systems to make them more reliable and secure, while work continues to fully replace older systems.
The residual risk currently scores 12 on a scale of 1 to 25.
Resources
Having the right funding and people in place is essential for the HRA to keep making progress and achieve meaningful results. If the HRA does not have enough financial or staff human resources, it may struggle to deliver its strategic priorities. This could be caused by reduced government funding, rising costs, or increasing national demands that expand the HRA’s work. There may be limits on staff capacity, gaps in skills, or weaknesses in planning and prioritisation.
If this risk occurs the HRA may not meet its strategic objectives and research approvals could be delayed. It could also reduce the UK’s ability to attract and support research, limit innovation and weaken international competitiveness. High workloads could lead to staff burnout and increased staff turnover, which would further affect the HRA’s ability to deliver its objectives.
The design and implementation of our target operating model will help address this risk alongside strategic workforce planning, strategic risk management and strategy delivery improvements to enable more adaptive management and coordination.
The residual risk currently scores 12 on a scale of 1 to 25.
Resilience
If the internal controls systems that keep the HRA resilient are not strong or well-aligned, the HRA may struggle to deliver its strategic priorities. This includes systems that protect against cyberattacks and help the organisation respond effectively if services are disrupted. These risks could arise from outdated or poorly maintained systems, weak access controls or poor data handling practices, staff who are not properly trained or insufficient backup and recovery arrangements.
The effects of this risk could disrupt research approvals and oversight, lead to loss of data integrity and availability, and potentially harm individuals through lost data. It could also result in breaches of UK data protection law, with possible fines or regulatory action and wider legal consequences. Failures in system resilience could also damage the reputation of the HRA and the wider public sector.
To mitigate this risk, the HRA uses a defence in depth approach to cyber security to protect our most important systems and information. Our arrangements are checked every year by the Government Internal Audit Agency, and we have been rated as providing a good level of protection. We also work with other government organisations to share information about cyber threats, monitor our systems on an ongoing basis and ensure our digital services meet government standards for security and protection.
The residual risk currently scores 12 on a scale of 1 to 25.
Performance analysis
Performance management
We plan our work to make our strategy happen. We do this by preparing an annual business plan, which sets out how we will turn our strategy into action. This plan is developed with the involvement of a wide stakeholder group, and is embedded throughout the organisation in our performance, people and risk management processes.
These processes help to make sure we successfully work towards our strategy by focusing on 24 key outcomes highlighted in the strategy and monitoring our progress in making these happen. Importantly, this also helps our people understand their role in delivering our plans.
We monitor and evaluate our performance against our strategy, business plan and financial plan every 3 months, and we collate a comprehensive performance report for our Executive Committee and Board to review. This includes focused performance metrics including user satisfaction data, an analysis of our change portfolio, a detailed performance report, risk management report and finance report. These reports combined provide assurance on how we are delivering our strategy, statutory functions and highlight areas for action and improvement.
Individual staff objectives that complement and support these organisational objectives are developed during the annual appraisal process and monitored throughout the year during regular one-to-ones between staff and their managers.
This year we strengthened alignment with the 24 strategic outcomes by appointing individual outcome leads, establishing a new information-sharing group to support delivery and working towards adapted governance and reporting arrangements.
The way that we manage our performance and its relationship with risk and uncertainty is explained in more detail in our corporate governance report on page 34.
As a learning organisation, we regularly review and refine our performance management and reporting systems, to ensure we focus on strategy delivery. We do this through continuous improvement activities such as lessons learned exercises as well as independent assurance activities including internal audit reviews.
We also set operational key performance indicators, which are collated and monitored by delivery teams, making sure we achieve our statutory requirements as well as continuously improving our services. Operational metrics are reported every 3 months to our Executive Committee.
Performance reporting
Our performance reporting focuses on 4 areas:
- customer satisfaction
- our services performance
- our people
- financial performance
User satisfaction
We measure how satisfied people are with our services by collecting feedback from those who use them. Overall satisfaction remains high with 84% of users saying they are satisfied or very satisfied with the service they receive. Users also rate their interactions with our staff very positively, with 94% reporting satisfaction or high satisfaction.
Online guidance is our lowest scoring area with 65% of users satisfied. Our Research Systems programme is modernising our digital services and will improve online information and guidance. As outdated systems are replaced, we expect user satisfaction in this area to improve.
Our services performance
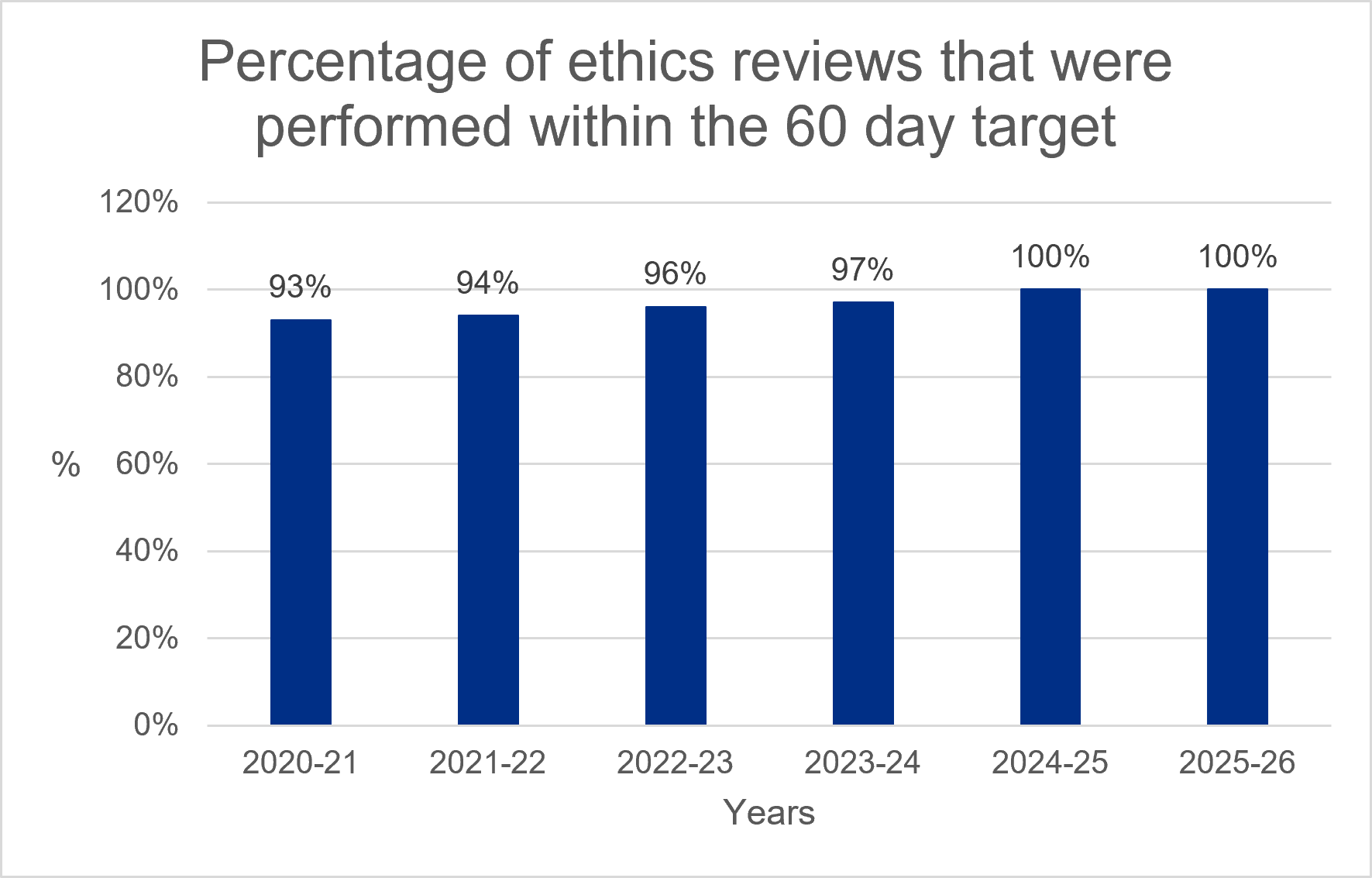
One important measure of our performance is the time it takes to conduct ethics review of clinical trials of investigational medicinal products (CTIMPs). Ethics review is provided by Research Ethics Committees (RECs) that assess research applications to determine whether they meet ethical standards. Our statutory performance target requires all ethical reviews of CTIMPs to be performed within 60 days. This graph sets out the percentage of reviews that were performed within this target. We are pleased to report that we have met our statutory performance target throughout the year, maintaining the improvement in this key metric achieved in 2024-25.
This year 4% of these reviews resulted in an unfavourable opinion. This is consistent with our previous experience.
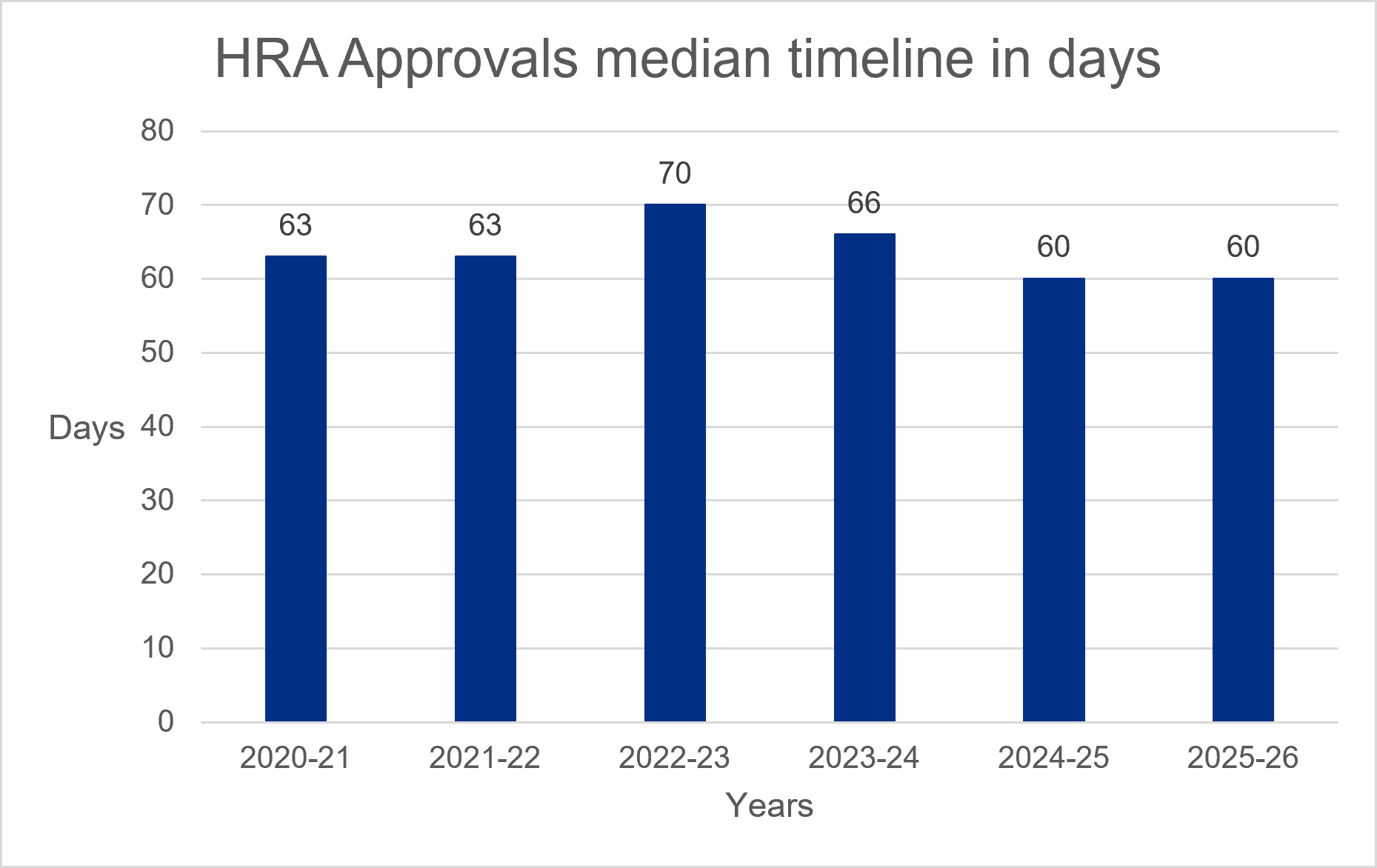
We also measure our performance by the median time it takes to deliver our HRA approval service, which remained at 60 days in 2025-26. This service brings together the assessment of governance and legal compliance, undertaken by dedicated HRA staff, with ethics review, performed by a Research Ethics Committee. This timeline is not completely within our control as parts of the process rely on other review bodies, coordinating organisations and researchers responding to queries to deliver a combined outcome to researchers. We work collaboratively with these organisations to make sure timelines are predictable and streamlined.
Our people
Our staff and HRA Community members show strong commitment to UK health and social care research. They keep our statutory services timely and high-quality and play a vital role in putting our strategy into action. We track their capacity to spot operational pressure points early so that we can put measures in place to maintain good services. We measure both staff and committee membership capacity to:
- compare our actual staff capacity compared to planned levels
- monitor our committee membership vacancy rate
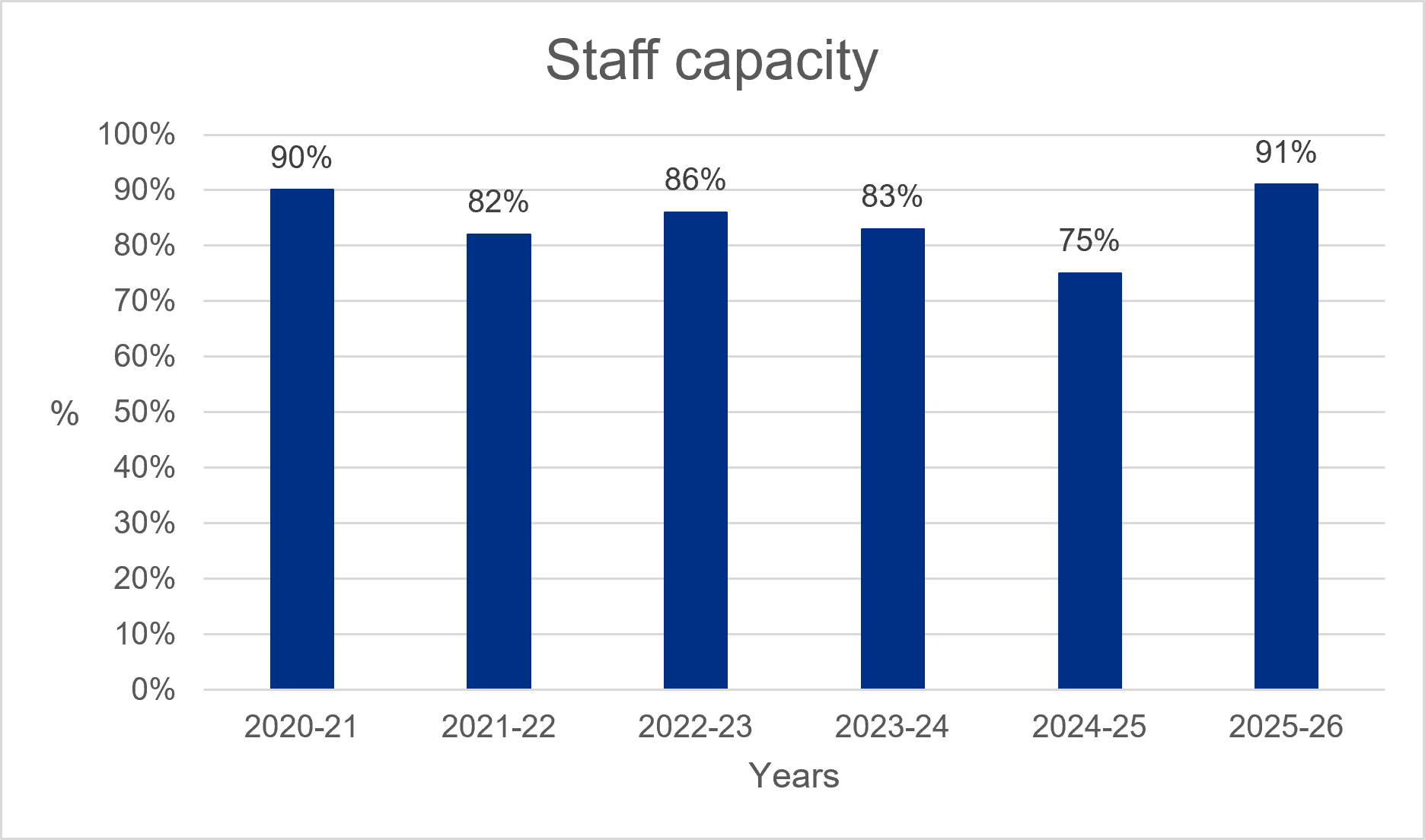
Staff capacity
Workforce planning is essential to make sure we can consistently provide our statutory services, put our strategy into action and respond to unplanned demands from the sector and UK government. This includes a careful assessment of our staffing, their skills and capabilities to make sure we have sufficient capacity to implement our planned work as well as respond to changes as they arise.
This year our staff numbers were closer to planned levels than in 2024-25 but we did not have enough people to fully meet our needs. Most of the gap was in digital roles needed for our digital transformation. There is strong competition for technical skills, a limited supply of specialists, and we needed to grow our digital capacity quickly for a short period of time. As a result, some roles were hard to fill or took longer than we had planned. This has slowed the pace of our Research Systems programme.
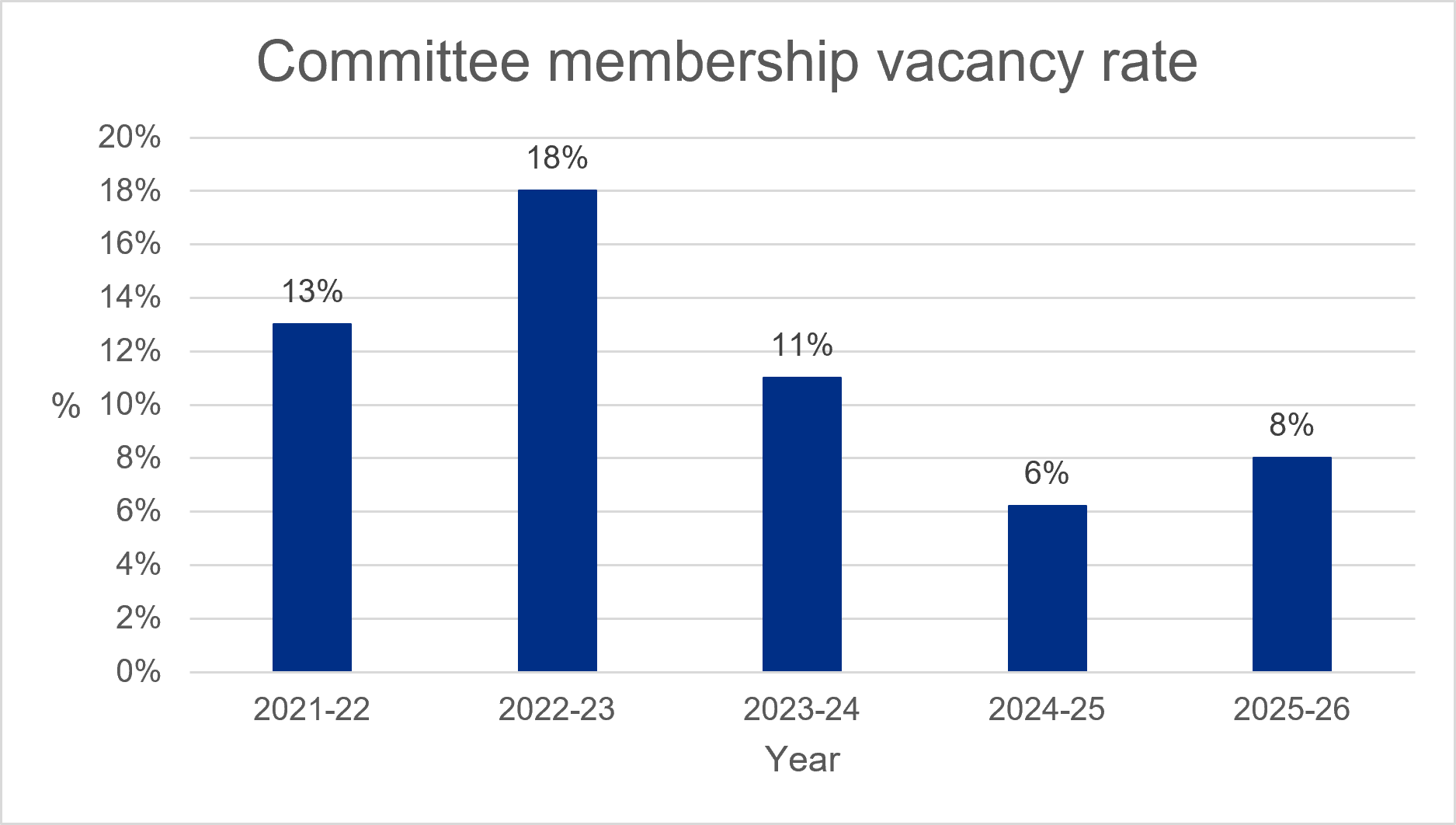
Committee membership vacancy rate
This year we have experienced a small increase in the committee membership vacancy rate although rates remain good and better than earlier years. We are not overly concerned with this recent change while we move away from old member classifications and allocate new designations to ensure quoracy and alignment with amended clinical trials regulations.
In 2026 we started to design a communications campaign to recruit new REC members with a strong focus on younger people aged 18-29 because currently, only 1% of REC members are under 30.
Financial review
Our accounts consist of our primary statements providing summary information about our income and expenditure in the year, our assets and liabilities at the end of the year, and how we have managed our cashflows. They also include detailed notes to these statements that provide more information about our accounts.
Our accounts have been prepared based on the standards set out in the Government Financial Reporting Manual (FReM) to give a true and fair view. We remained within our agreed revenue and capital funding allocations for the Department of Health and Social Care (DHSC) for the year-ended 31 March 2026.
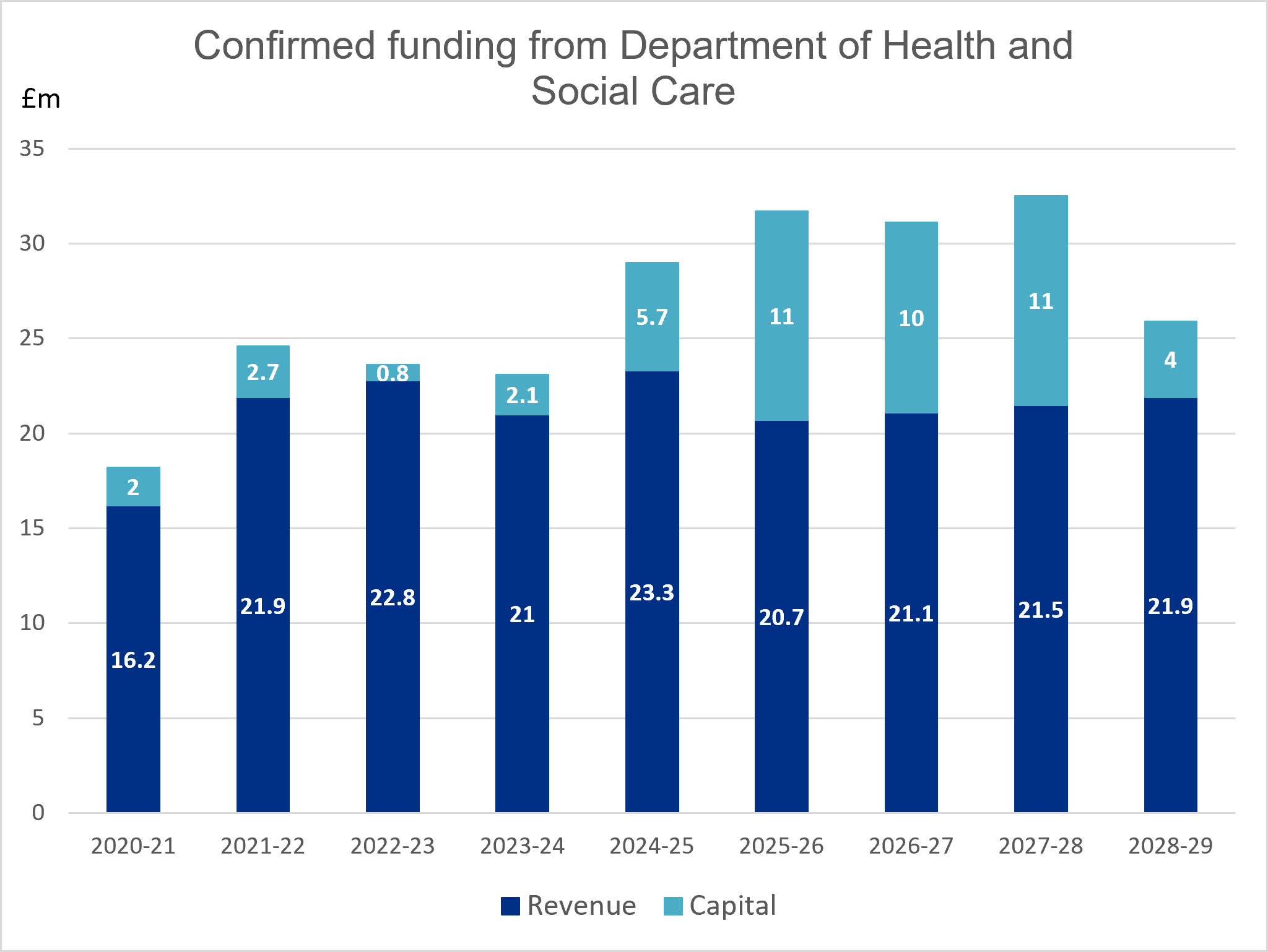
Government funding
Our total confirmed funding from DHSC for the year was £31.7m (2024-25 £29.0m), of which:
- £20.7m (2024-25: £23.3m) was revenue funding
- £11.0m (2024-25: £5.7m) was capital funding
Funding received from DHSC in year was £24.3m (2024-25 £24.8m) due to changes in our digital transformation profile shifting expenditure into future years.
This year, we have maintained 10% efficiency savings delivered through our 2024-25 Adapt and Change programme. These savings helped manage rising costs that were not covered by funding and created capacity to invest in our digital transformation. In total, we reported £1.6m in ongoing savings in core costs to DHSC. We achieved these savings by reducing our property footprint, stopping non-statutory services, reshaping teams and making greater use of shared public sector services. The programme finished earlier than planned, allowing savings to be realized 6 months ahead of schedule.
These savings, together with the increased funding confirmed through the recent spending review, will enable us to replace and modernise our research digital services. They will also support our transition to a new target operating model, focused on creating value more quickly for the research sector and improving decision making.
Our digital transformation will help strengthen the UK’s position as a global leader in life sciences. It will also support the NHS by making research approvals easier, faster and more cost-effective. The funding for this work has been approved by DHSC Investment Committee and confirmed through the spending review process.
Increased funding between 2021 and 2023 supported the successful launch of our combined review service, developed in partnership with MHRA. Introduced in January 2022, this service allows researchers to apply for both ethics and regulatory approval through a single application. On average, it has reduced approval times by around 50%.
In 2022-23 we paused our digital transformation to review our approach and learn from the introduction of combined review. This pause reduced the funding needed in 2022–23 and 2023–24, particularly for capital investment. As part of the DHSC Efficiency and Reform Review, we agreed to delay activity to ensure the programme was properly set up for success, which reduced costs in those years. The programme was relaunched in autumn 2023, with funding increasing to support delivery.
Other revenue
We also received income from cost-sharing arrangements with other publicly funded organisations, which included:
- £0.65m (2024-25: £0.39m) from the devolved administrations for providing support and digital systems to deliver the UK research ethics service
Future funding
The Department of Health and Social Care have confirmed our revenue funding for 2026-27 is £21.1m and our capital funding is £10.0m.
How do we spend our funding?
We carefully plan our work to make sure we deliver our strategy effectively. Our business planning process helps us decide how best to use our limited resources so we can achieve the greatest impact. It ensures that we spend public money wisely, based on the funding we have been given. During the year, we may not use all available funding if plans change, are delayed, or if savings are made.
Our total revenue spending for the year was £20.7m (2024–25: £20.2m), this was slightly lower than planned, due mainly to delays in bringing in new staff and skills needed for our Research Systems programme, which reduced staff costs compared to plans. We also spent less than expected on software licences, and a change in how VAT was treated following an independent review reduced costs further. In addition, amortisation costs were lower than planned, reflecting changes in when digital assets are considered fully in use.
Most of our spending (71%) relates to staff costs of £14.7m (2024–25: £15.3m, 76%). Our staff are paid in line with NHS Agenda for Change pay scales and terms and conditions. Our staffing structure is agreed through the annual business planning process. Any changes to this structure must follow our formal financial approval and business case processes.
Making payments
We aim to comply with Better Payments Practice Code by paying suppliers within 30 days of receipt of an invoice and our performance is shown in the tables below.
| Non-NHS by number of invoices |
2025-26 Number |
2024-25 Number |
| Total non-NHS invoices paid in the period | 886 | 893 |
| Total non-NHS invoices paid within target | 878 | 882 |
| Percentage of non-NHS invoices paid within target | 99.1% | 98.8% |
| NHS by number of invoices |
2025-26 Number |
2024-25 Number |
| Total NHS invoices in the period | 81 | 94 |
| Total NHS invoices paid within target | 81 | 94 |
| Percentage of NHS invoices paid within target | 100.0% | 100.0% |
| Non-NHS by invoice value |
2025-26 Value ‘£000 |
2024-25 Value ‘£000 |
| Total non-NHS invoices paid in the period | 10,154 | 8,092 |
| Total non-NHS invoices paid within target | 10,150 | 8,092 |
| Percentage of non-NHS invoices paid within target | 100.0% | 100.0% |
| NHS by invoice value |
2025-26 Value ‘£000 |
2024-25 Value ‘£000 |
| Total NHS invoices paid in the period | 2,088 | 1,917 |
| Total NHS invoices paid within target | 2,088 | 1,917 |
| Percentage of NHS invoices paid within target | 100.0% | 100.0% |
Strategy performance analysis
This section covers how we are performing against our objectives in our strategy 2025-28.

Here we have set out how you will see us work in this way, with measurable outcomes that we will achieve over the next 3 years and our progress so far.
Simple: We need to be simple for researchers to find out how to do research with and for everyone and access support to this well
Strategic outcome: make it easier to do research across different settings in the UK, broadening access to research
Measurable outcome:
- 10% increase in the percentage of people who tell us that it is easy to set up studies in the UK including across NHS and non-NHS settings
Performance:
- we set the baseline data for this measure which will be achieved by 2028 using an annual survey, and published the results on our website
- we explored barriers to carrying out research in non-traditional settings and co-produced a report on governance outside the NHS
- we introduced more proportionate ways of managing research, helping studies run more easily across multiple organisations
Strategic outcome: researchers have a positive experience when finding out about what they need to do and earning the approvals that they need
Measurable outcome:
- 75% of applicants rate our overall service highly
Performance:
- we exceeded this benchmark; 84% of applicants provided high ratings for our overall service
Strategic outcome: make research more transparent
Measurable outcome:
- 100% registration of clinical trials and an increase in clinical trials uploading a summary of results on a registry, including across NHS and non-NHS settings
Performance:
- 94% registration of clinical trials (or in the process of registration) achieved, an increase of 2% on the previous year’s data.
- research transparency compliance data is available on our website
- to encourage awareness, we actively contacted sponsors one year after their research approval to check if they had registered their study.
- we also contacted sponsors who had not submitted their final report and by doing so, increased reporting by 8% to 68%.
Strategic outcome: ensure that more research meaningfully involves the public to inform the way it is done
Measurable outcome:
- increase in rates of public involvement in applications for review by a Research Ethics Committee (REC)
Performance:
- we set the baseline data for this measure using data published from 2023 and 2024 on rates of public involvement in applications for review by RECs
- we are analysing the data from 2025 and will publish our findings in 2026
- we lead the shared commitment to public involvement and the group continues to grow and flourish with 38 partners taking part
Strategic outcome: support greater representation in, and access to, research so that people from all backgrounds across the UK can take part in research relevant to them
Measurable outcome:
- increase in the proportion of researchers who use an Inclusion and Diversity Plan and are more confident to include a diverse group of people in their research
Performance:
- we piloted draft guidance to develop an Inclusion and Diversity plan with the MHRA and are now reviewing the results
- these findings will also inform how we will develop measures on the use of plans by researchers and sponsors
Strategic outcome: support researchers to do research in new ways and using new technologies such as AI to improve care in a way that people can trust
Measurable outcome:
- be clear how we support researchers to use new technologies and data to plan and do research, and to research the use of new approaches and technologies in care, in line with the Artificial Intelligence (AI) Opportunities Plan
Performance:
- measurement for this strategic outcome has not yet been established given the emerging nature of research involving new technologies
- we developed a set of commitments aimed at enabling researchers to undertake studies involving AI and other emerging technologies within a trusted regulatory framework
- these commitments form the foundation for future work, which will be reported to the Department of Science, Innovation and Technology to support innovation in research methods and technologies while ensuring studies involving AI continue to meet ethical and governance standards.
Fast: We need to be fast to plan, approve, set up, manage and complete research in the UK
Strategic outcome: provide approvals in time to support the set-up of clinical trials in 150 days
Measurable outcome:
- provide 100% approvals of clinical trials within a maximum of 60 days, with a median timeline below 40 days
- ensure that you get a decision on support for the use of confidential patient information without consent in England and Wales from the Confidentiality Advisory Group within 60 days or where a precedent has been supported, within 30 days
- ensure that all research applications will receive a HRA and HCRW Approval decision in less than 60 days
Performance:
- we provided approvals for 100% clinical trials within 60 days, with a median of 30 days
- we completed 99% CAG decisions for full review within 60 days and 86% of precedent set reviews within 30 days
- we confirmed an HRA and HCRW approval decision within 60 days for 59% of all research applications received. HRA and HCRW approval can only be issued once all regulatory approvals are in place and applicants have responded to requests for information
Strategic outcome: make setting up research more efficient, with simple steps and no duplication
Measurable outcome:
- reduce the burden, time and cost to do research by standardising processes and reducing duplication in the set-up of research studies, with a 20% increase in the percentage of people who tell us that the process of study set up is efficient
Performance:
- we set baseline data for this measure which will be achieved by 2028 using an annual survey, and published the results on our website.
- we worked with a wide group of partners from across the sector to understand where duplication exists and how efficiencies can be made
- we are now translating this learning into initiatives, such as our mandated agreements, to bring improvements over the strategy
Strategic outcome: make it faster and easier to use our new digital services to plan, approve, set up, manage and complete research in the UK
Measurable outcome:
- we will reduce the burden on users by improving end-to-end flow and replacing manual processes including delivering 3 core platform services by 2027
Performance:
- we introduced the first users to our new digital service, plan and manage health and care research; they are now using it to submit and approve modifications to eligible study types
- we continue to design, build and release new functionality
Trusted: We need to be trusted by everyone who needs us
Strategic outcome: ensure that our digital services are secure
Measurable outcome:
- we will maintain and increase the security of our digital services, keeping them available and resilient to cyber-attacks and meeting government assurance standards
Performance:
- we successfully met the expected standards in the Data Security and Protection Toolkit, an online self-assessment tool that allows organisations to measure their performance against the National Data Guardian’s 10 data security standards
- we participated in cross-government threat intelligence and security networks, implemented continuous monitoring and made sure our digital services meet government security and data handling standards
Strategic outcome: ensure that people can understand, value and trust us and the way that we work
Measurable outcome:
- better understand who needs us, what they need from us and why they need it to inform how we work, so that sentiment analysis will show an increase in awareness and trust in the HRA across all stakeholders that need us
- meaningfully involve people in the HRA’s work with at least 80% telling us that they feel that they had shaped and informed the work they had been involved in
- make sure that an increasing diversity of perspectives inform our work by setting objectives for where we want to increase representation in our work and working to achieve this
Performance:
- we received feedback from 40 people and 90% told us that they felt they had shaped and informed the work they had been involved in
- we defined personas for HRA stakeholders and conducted a sentiment analysis, the findings of which will be used to make decisions over how to build a profile that we need to achieve our objectives well, informing activity in 2026-27
- we worked with partners across the UK to improve how we collect and monitor demographic data include REC members, and engagement with under-represented groups to help us take action to improve inclusion
Strategic outcome: ensure that our assurances are understood, valued and trusted, and not unnecessarily repeated to set up research
Measurable outcome:
- 20% reduction in percentage of people who tell us that there is duplication in study set up
Performance
- we held qualitative interviews to better understand the personas that we need to engage with to ensure that our assurances are understood, valued and trusted
- this foundational work will inform targeted campaign activity in 2026-27 focused on increasing awareness of our assurances among these personas
Strategic outcome: ensure that people know when and how to raise questions and concerns with us and we are clear how we will act on them
Measurable outcome:
- 100% of complaints completed in 25 days and not more than 5% resulting in a subsequent appeal to the Chief Executive
Performance:
- we fully met this performance measure
Effective: We need to be effective taking action to improve the research system and support our people well
Strategic outcome: develop safe, scalable and secure digital infrastructure
Measurable outcome:
- we will build safe, scalable and secure digital infrastructure and the internal capability to expand, innovate and support future regulatory change
Performance:
- we developed our digital target operating model and planned how it would be implemented
- we implemented the first phase of our new digital service management tool improving user experience and service resilience
Strategic outcome: use Artificial Intelligence (AI) well
Measurable outcome:
- we will use AI and digital technologies well and find ways to use them more to improve the way we work and our services in a way that people can trust
Performance:
- we made Copilot available to all staff supported by training, guidance and policies.
- we explored how Copilot might further streamline workflows and automate basic processes.
- we increased our capability to use AI in our digital service management
Strategic outcome: ensure that our staff have a high level of engagement
Measurable outcome:
- maintain and grow our high level of staff engagement to 80% and maintain our strive measure at 85%
Performance:
- our staff engagement score in 2026 is 77% and improvement of 3% on 2025 (74%)
- we put in place an action plan to respond to our 2025 staff survey, organised around 3 key themes; valuing people, developing people and supporting people well through change
- key actions achieved include the introduction of a staff recognition scheme, our Stepping into Leadership programme, training a group of staff to be mentors and coaches, a new buddy scheme for new joiners and our first secondment policy
Strategic outcome: ensure that our community of volunteers and public contributors have a good experience with us and can see the difference they make
Measurable outcome:
- maintain satisfaction rates at or above 80%
Performance
- we exceeded this measure and achieved over 80% satisfaction from our community members in our 2026 survey
- we plan actions to address feedback from this survey which is repeated every 2 years
- our 2024 action plan is available on our website
Strategic outcome: play our part in reducing government running costs
Measurable outcome:
- play our part in meeting the commitment for government departments to reduce their administrative budgets by 15% by the end of the decade
Performance
- we made £1.6m annual efficiency savings through our Adapt and Change programme
we reported on our progress to DHSC every 3 months
Sustainability report
The HRA is committed to environmental sustainability and achieving net zero. To help make this happen, the Green team - a staff-led group committed to improving sustainability - developed and launched our first Environmental sustainability strategy in 2022. This strategy embeds environmental sustainability in our culture and ways of working and was updated in 2025.
We have made good progress this year with continued emissions monitoring and increased awareness of our Environmental sustainability strategy. We are pleased with how much we have achieved and want to do more to make sure we play our part ensuring the environment is protected for future generations.
We work in partnership with our colleagues at the Department of Health and Social Care (DHSC) and our Green team, to improve environmental performance across the organisation. Our strategic priorities are to embed environmentally sustainable practices into our daily business, making environmental sustainability the norm, and encouraging and facilitating sustainability in research.
Our work is aligned with the 5 environmental principles, as set out in section 17(5) of the Environment Act, encouraging not only our teams but also our partners and suppliers to consider the environment in all activities.
Our estates strategy works alongside our environmental sustainability strategy to support our HRA-wide strategy. This includes ensuring that sustainability and environmental performance is prioritised in decision making. We also make sure lease events are managed, meeting government policy and supporting our strategy. In 2025, we reduced our 5 office locations to 4 ensuring we were in spaces shared with other government bodies such as the Care Quality Commission (CQC) to improve office utilisation and energy efficiency.
Where we share offices, energy reporting is provided by our public landlord and is included in our Greening Government Commitment reporting.
Several initiatives have continued including:
- looking at how we buy goods and services to make sure sustainability considerations are included in decision-making
- introducing an Environmental sustainability statement in all new policies and procedures
- assessing all domestic and international flight requests against several factors including cost, time, energy consumption and staff wellbeing before booking travel
The following tables show our key performance indicators that help us measure our ambition to achieve net zero.
Carbon Dioxide (CO2) emitted by rail travel – staff
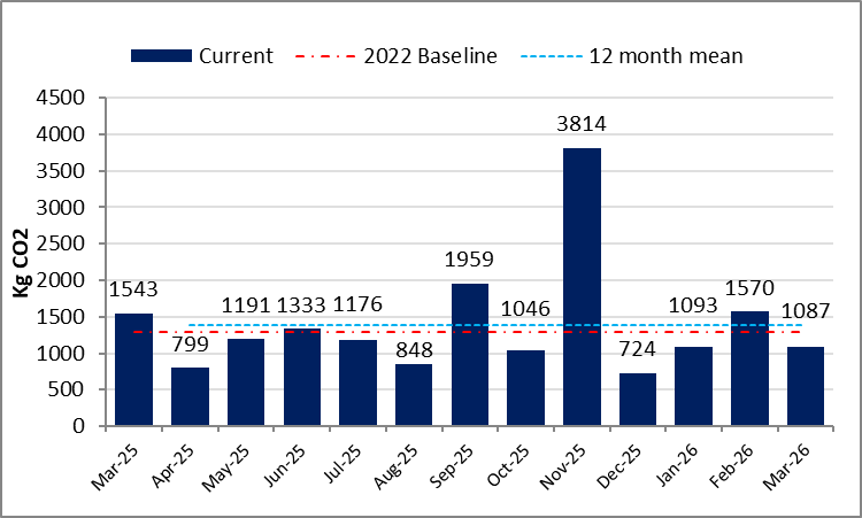
The graph shows monthly carbon dioxide CO2 emitted from rail travel undertaken by staff from April 2025 to March 2026. Emissions were highest in November 2025, reflecting an in-person meeting attended by over 100 staff, which was important for our operational effectiveness. The 2022 baseline and our target for CO2 is shown in red at just below 1,500 KgCO2. Our staff travel in 2022 was significantly lower than pre-pandemic levels and travel this year was slightly above this target. We set this target as a stretch target for 2025, unsure what our future travel requirements would be following the pandemic. We are closely monitoring our staff travel so we meet both our sustainability goals and make sure our people can work well.
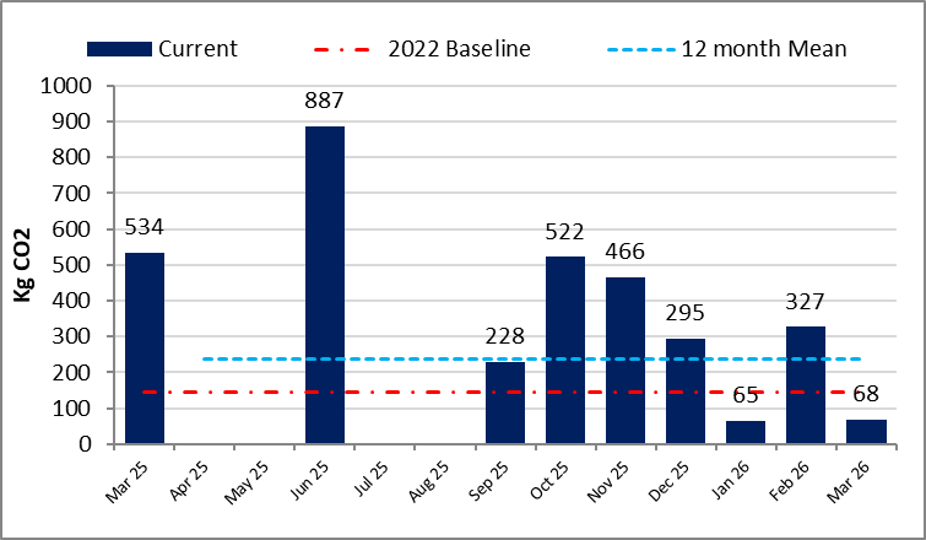
CO2 emitted by rail travel – Committee members and public contributors
The following graph shows monthly carbon dioxide (CO2) emitted from April 2025 to March 2026 through rail travel undertaken by committee members and the public who are involved in our work. The 2022 baseline and our target for CO2 is shown in red around 150 KgCO2. Again, this level was set as a stretch target and will be monitored closely to help us set a realistic target for future monitoring.
Carbon Dioxide (CO2) emitted by rail travel – Committee members and public contributors
Staff and HRA Community domestic flights – cumulative CO2
There were no domestic flights during 2025-26.
Dr Matthew Westmore
Chief Executive
Health Research Authority
29 June 2026